
Your Kid Hit Their Head. Now What?
How Pediatricians Think Through Head Injuries

It happens in slow motion and all at once. One second your toddler is climbing the couch, and the next thing you know you're kneeling on the floor with your heart in your throat, watching them cry—or worse, go eerily quiet. Or maybe it's your 10-year-old coming off the soccer field after a collision, holding their head, and you're trying not to panic but wondering: do we go to the ER right now, or is this okay?
Head injuries in kids are one of the most anxiety-provoking things for parents. The stakes feel enormous, the symptoms can be confusing, the internet is full of conflicting advice, and you constantly second-guess your instincts.
But pediatricians have tools that help us decide if a child is at serious risk for complications following a head injury. And I think learning some of the pillars that make up that framework can lessen parental anxiety, and increase confidence in making these decisions.
First Question: Is This an Emergency?
The reassuring news is that the vast majority of childhood head injuries are not emergencies. Most are mild, most children recover completely, and most do not require a CT scan or a trip to the ER.
But some do. And that is where the anxiety creeps in. So knowing the signs that make pediatricians more concerned is invaluable.
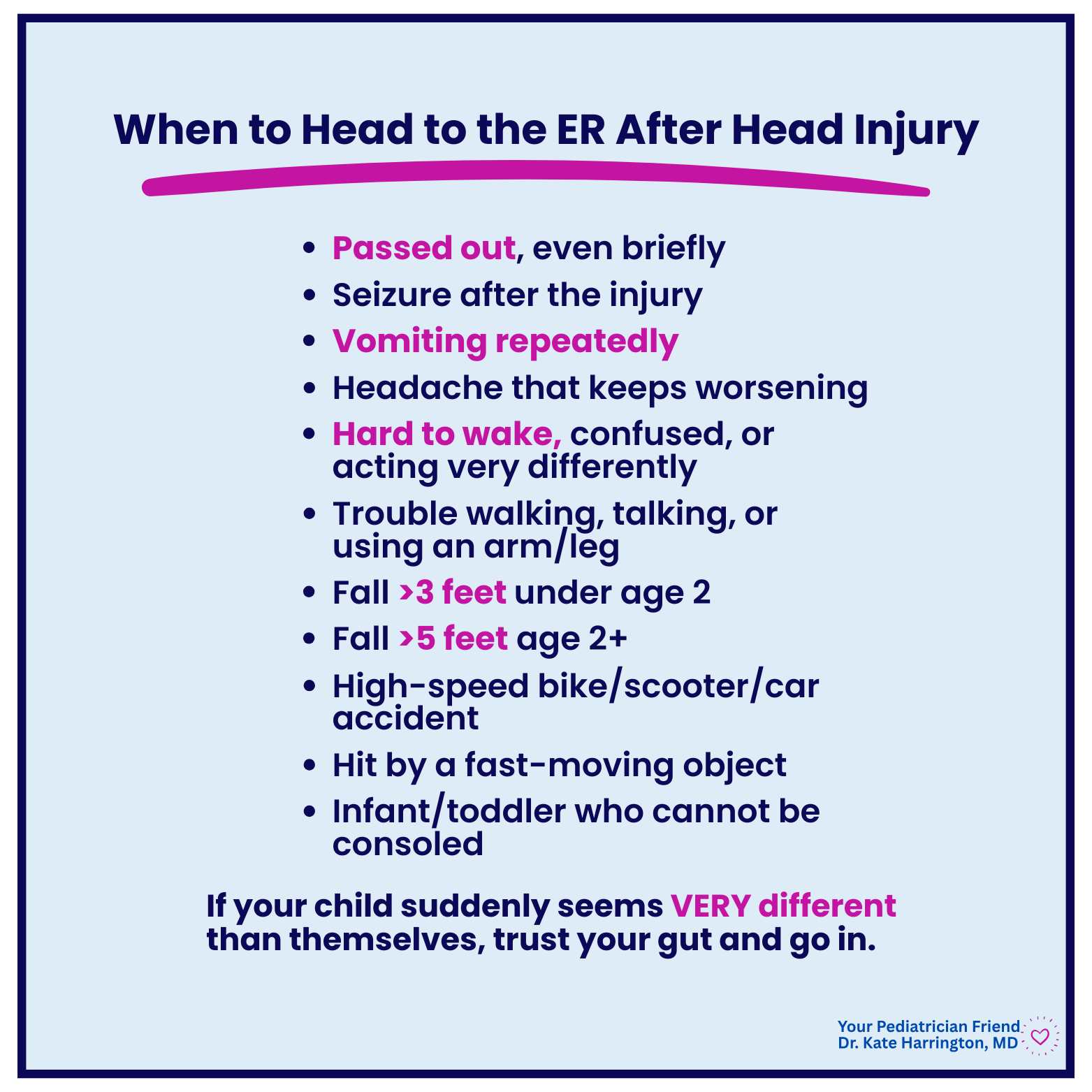
Go to the ER Now If Your Child Has Any of These:
Passed out, even briefly
Seizure after the injury
Repeated vomiting (one episode can be normal; multiple episodes is concerning)
Headache that keeps getting worse rather than stabilizing or improving
Hard to wake up, confused, or acting very different from their normal self
Trouble walking, talking, or using an arm or leg
A fall from more than 3 feet in a child under age 2
A fall from more than 5 feet in a child over age 2
High-speed mechanism—high-speed bike accident, car accident, fall from significant height, hit by a fast-moving object
An infant or toddler who cannot be consoled
And always, trust your gut if it says something is wrong. You know your child better than anyone else. And if they seem very different from themselves, get them seen.
A Special Note on Infants
If your baby under 12 months rolls off a changing table or falls from a caregiver's arms, the panic that follows is intense. But generally if they cried immediately, are consolable, and are acting normally within a few minutes, that's reassuring. Any infant who seems unusually sleepy, won't feed normally, is inconsolable, vomits, or had any period of limpness or unresponsiveness after a fall should be seen right away. When in doubt with a baby this young, call your pediatrician or go in—the threshold is lower and we’d rather talk it through.
The Middle Ground: Call Your Pediatrician
Not every head injury is an ER situation, but not every one is purely watch-at-home either. Call your pediatrician if your child:
Had a brief headache that has since resolved but you're still feeling uneasy
Seems a little "off"
Is older and complaining of symptoms you're not sure how to interpret
Had any loss of consciousness, even briefly, but is now acting normally
Your pediatrician can help you decide whether your child needs to be seen, and when. We’d rather you reach out than sit at home and worry!
What's Actually Happening in the Brain During a Concussion
Despite what most people think, a concussion is not just the brain getting "shaken up."
When the brain sustains a concussive impact, a whole cascade of physiological events is triggered. The rapid movement of the brain inside the skull (yes, the brain actually moves) disrupts the normal electrochemical environment of brain cells. There's a sudden release of neurotransmitters, a shift in ion balance across cell membranes, and a period where brain cells are working harder but getting less blood flow to fuel them. Think of it as an energy crisis at the cellular level. That’s why kids can feel foggy, exhausted, emotional, dizzy, or slow after a concussion, even when imaging is normal.
Signs That Make Me Think Concussion
No single symptom confirms a concussion—it's always a constellation of findings. But here are the symptoms that, after a head injury, make me more suspicious of a concussion (and I’d want you to reach out to your pediatrician):
Mental fog or feeling "out of it"
Headache, especially one that persists or worsens
Dizziness, balance problems, or unusual clumsiness
Drowsiness or unusual fatigue in the hours after the injury
Nausea or repeated vomiting
Sensitivity to light or noise
Memory problems, including not remembering the injury itself or events just before or after it
Trouble focusing the eyes or tracking objects
For older children and teens, we also watch for emotional symptoms like irritability, sadness, or feeling "not right.” These are often underrecognized parts of a concussion.
Recent research has shown that if your child has no headache after a head injury, they are much less likely to have suffered a concussion. So, a general rule of thumb is if they have no headache, are acting like themselves within an hour or two, and are walking and talking normally, a concussion is less likely.
🩺 Pediatrician’s Insight: One of the biggest misconceptions about concussions is that a child has to “black out” for it to count. Many kids with concussions never lose consciousness.
How Doctors Make Decisions After a Head Injury
Are you ready for the inside information I promised you?
When a child comes into the emergency room or clinic after a head injury, a doctor is working through a mental checklist and assessing your child as soon as they walk in the room. Two validated clinical tools are helping them make decisions: the Glasgow Coma Scale (GCS), which assesses level of consciousness, and PECARN (the Pediatric Emergency Care Applied Research Network rule), which helps determine whether a CT scan is actually needed. PECARN was developed after analyzing more than 42,000 children across 25 hospitals and is one of the most widely used decision tools in pediatric emergency medicine.
Generally, a doctor is reassured if your child:
is fully alert and acting like themselves
has no persistent or worsening headache
has vomited no more than once
was injured by a low-energy mechanism (bumped a cabinet, rolled off the couch, short fall onto carpet, fell from their own height).
These children are very unlikely to meet criteria for imaging.
A doctor is more concerned if a child:
lost consciousness, even briefly
has a headache that is worsening rather than improving
has vomited more than once
seems confused or "off"
was injured by a high-energy mechanism like a car accident, a significant fall, or a high-speed collision.
These children are more likely to need further evaluation, and may need a CT scan.
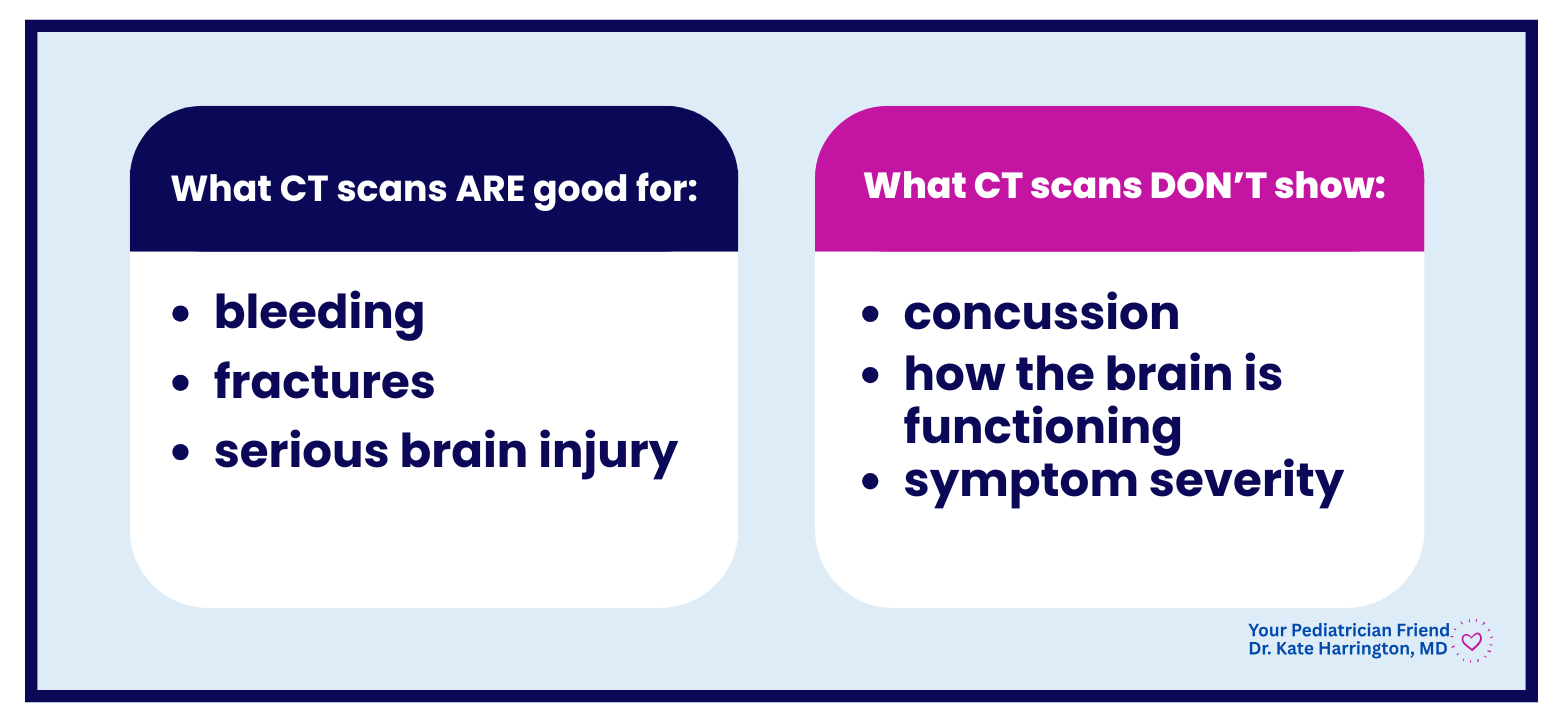
CT scans are excellent at detecting bleeding, fractures, and structural brain injury, but they cannot show a concussion—a concussion is a functional disruption rather than a structural one. So clinical evaluation and observation will almost always matter more than imaging alone.
💡 Fun Fact: The original PECARN study found that roughly 1 in 5 children over age 2 who received CT scans after head trauma were in the very-low-risk category and didn't actually need them. This is important because CT scans expose children to ionizing radiation, and the developing bodies and brains of children are more sensitive to radiation than adults.
Do I Need to Wake Them Up?
This is one of the most common questions I get when I talk to people about head injuries. And it's one where grandma’s advice differs from ours. The short answer: usually, no.
The origin of "wake them every hour" advice comes from an era before we had good clinical tools to identify children who are truly at risk for bleeding into the brain. The fear was that a child could go to sleep and deteriorate overnight from a growing bleed.
If your child had a concerning enough injury that we were worried about bleeding into the brain, there would usually be additional warning signs like those discussed above, and they should be evaluated in the ER before sleep. If your child has been evaluated (or clearly meets the reassuring criteria above), is acting like themselves before bed, and is recovering normally, you do not need to set an alarm every hour.
I usually tell parents to check on your child before you go to sleep. Glance at them, and if they look comfortable and are breathing normally, let them sleep. Sleep is actually beneficial for brain recovery—disrupting it through the night is more likely to hurt than help.
If your child is unusually difficult to rouse, is breathing abnormally, or something seems wrong when you check, that's when you call or go in.
Getting Back to Normal
Kids with concussions do not need to be in a dark room, on total rest, doing nothing.
The old "cocoon therapy" approach (strict bed rest, no screens, no stimulation until all symptoms are gone) has been largely disproven. (Again, changing data over the years is what makes head injuries especially hard to manage as a parent—what grandma knew and practiced is now no longer standard care.) Current guidance from the CDC and AAP supports relative cognitive rest in the first day or two, followed by a gradual return to activity.
Generally okay in the first 48 hours:
Coloring, drawing, Legos, puzzles
Short walks
Audiobooks
Quiet play and calm social time
Short screen time if symptoms stay stable
Try to avoid:
Contact sports and roughhousing
Trampoline parks, roller coasters, activities with re-injury risk
Long, high-intensity screen sessions that worsen symptoms
Anything that makes symptoms noticeably worse
A useful rule of thumb: if an activity makes symptoms worse, stop and rest. The brain is telling you something.
Return to School First
Most children can return to school within 1 to 2 days of a concussion, even if they're still experiencing some symptoms. This is not pushing too hard; it's actually supported by research showing that getting back into normal routines can shorten recovery and reduce the likelihood of lingering emotional symptoms.
The key is going back with accommodations, if needed. Common supports include extra time on assignments, a reduced schedule on hard days, preferential seating away from bright lights, and the option to take breaks when symptoms flare. Your child's doctor can write a letter to the school outlining these needs.
Then Return to Sports
Before returning to full contact sports after a concussion, your child needs to be cleared by their healthcare provider. The standard return-to-sports protocol is a step-by-step progression:
Symptom-free at rest
Light aerobic activity: walking, easy swimming, no resistance training
Sport-specific exercise: skating drills, soccer drills (but no head contact)
Non-contact training drills
Full-contact practice (only after medical clearance)
Return to competition
Each step requires roughly 24 hours of no symptom recurrence before moving to the next. If symptoms return at any stage, go back a step.
When in doubt, sit them out. That's not being overprotective or mean! Your child’s brain health is much more important than a game.
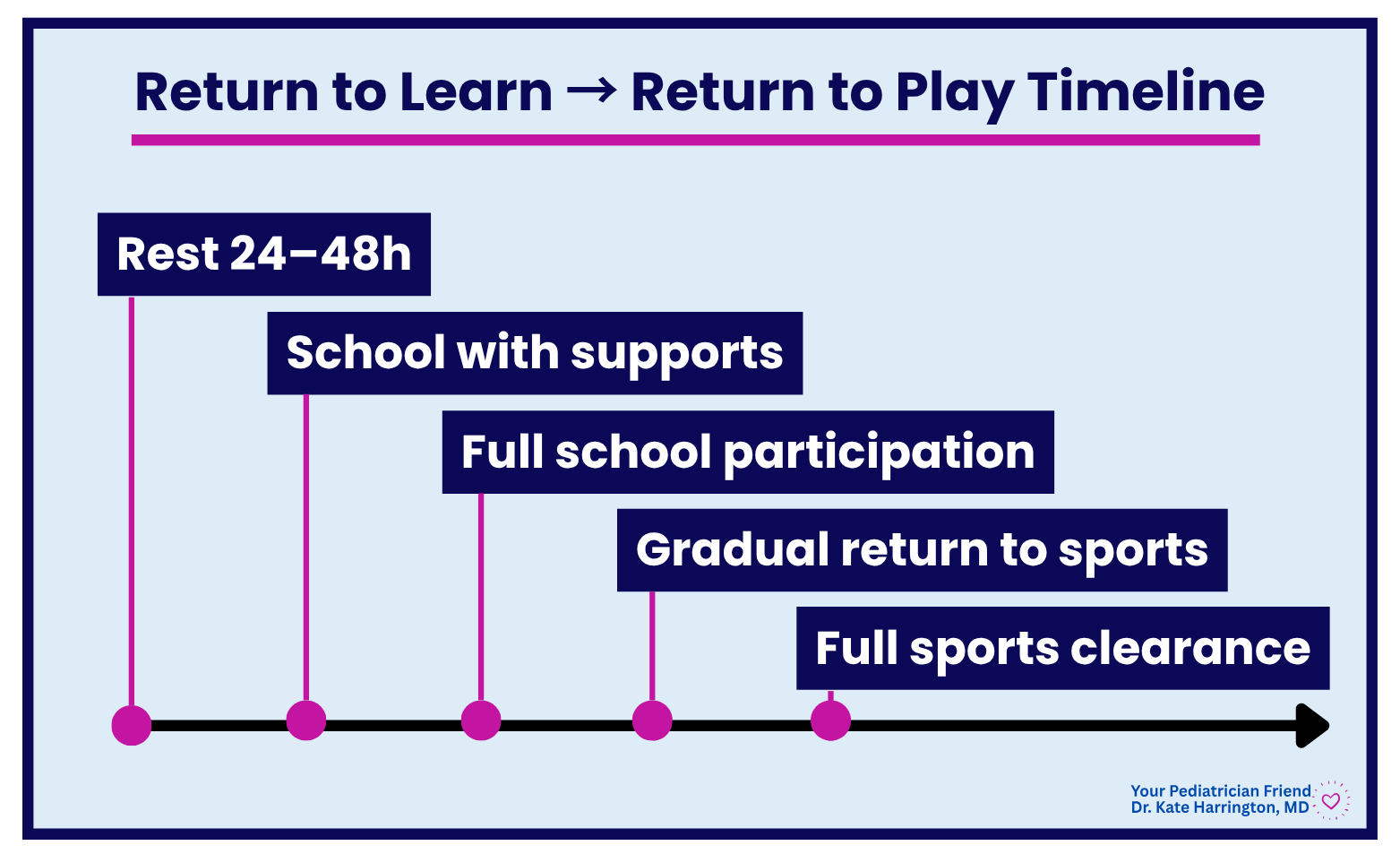
🩺 Pediatrician's Insight: The sequence that matters here is return to learn, then return to play. Kids should be tolerating school and daily activities (thinking without symptoms worsening) before they return to contact sports. This is because the developing brain needs to have recovered functional capacity before it takes on risk of re-injury. Second-impact syndrome (a second concussion before the first has healed) is rare but serious, and it's far more likely in someone who returned too soon.
A Note About Recovery Time
Most children with a concussion will feel better within a couple of weeks. Some children, particularly adolescents, take longer—sometimes four to six weeks. A small percentage have symptoms that persist beyond a month, which is called post-concussion syndrome and warrants a more thorough evaluation. Factors that can extend recovery include a prior concussion history, migraine history, anxiety or depression, and returning to play too soon.
💡 Fun Fact: Research has found that adolescent female athletes tend to report concussion symptoms at higher rates than their male counterparts in sports played by both sexes, like soccer and basketball. This may be related to differences in neck muscle strength (which affects how much the head moves on impact) and possibly hormonal factors, though research in this area is ongoing. It's one of the reasons concussion protocols in girls' sports deserve the same rigor as in boys' contact sports.
The Bottom Line
The great news for parents everywhere is that most childhood head injuries are not emergencies. Most concussions recover completely. The key is knowing:
When to go in now (the red flag list above)
What a concussion actually looks like
What the clinical tools we use are (PECARN, GCS—now you know!)
What actually helps (relative rest, early return to school, graduated return to sports)
I hope you never need this. But we know kids fall and collide and tumble…it's part of childhood whether we like it or not! Save this for the next playground fall, soccer collision, or bike wipeout.
Head injuries are scary because our kids’ brains feel precious to us—and they are! But most childhood concussions heal completely with time, support, and patience. And when you're not sure, reach out to a pediatrician. That's exactly what we're here for 💕