
The RSV Timeline: What to Expect Each Day
A pediatrician’s day-by-day guide to one of the most stressful viruses of early childhood
It’s that time of year when we start seeing RSV cases creep up. Historically, this has been one of the hardest times of the year for me as a pediatrician because RSV is sooo stressful for parents.
It just changes so quickly. One minute your baby simply has a runny nose…and 36 hours later you are dealing with SO much mucus, worried about your baby being dehydrated, and wondering if you should head to the ER.
And parents who have had a baby with a rough case of RSV definitely have PTSD—it is that stressful!
But, one helfpul thing we can do is be prepared. Know what the typical timeline is, and when you need to be worried.
So, let’s walk through it!
A Quick Refresher: What Is RSV?
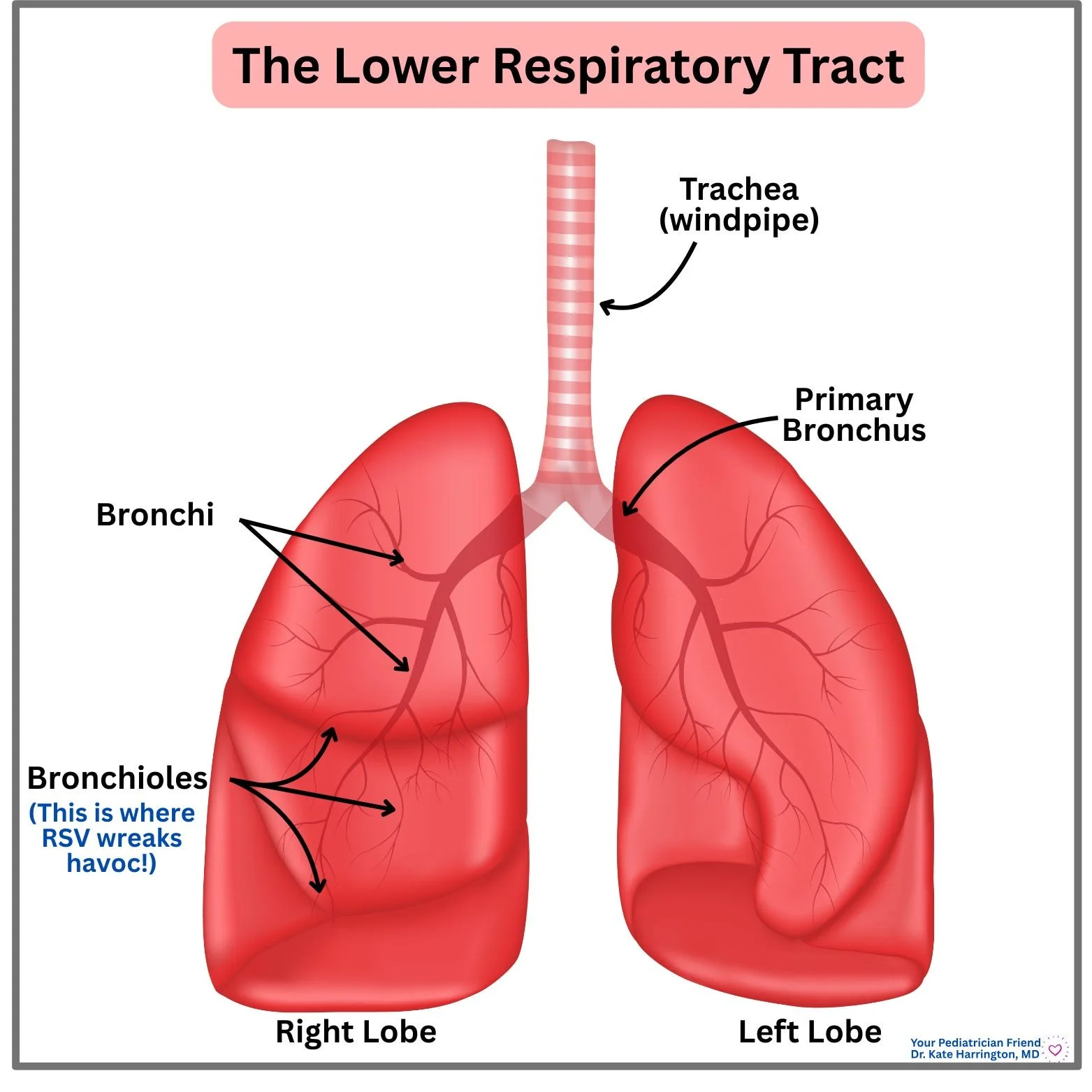
RSV (or respiratory syncytial virus) is a very common respiratory virus. In fact, almost all kids will have their first infection with RSV by the time that they are 2 (and unfortunately, you read that right: you can get it more than once). It causes congestion (like buckets of congestion), cough, and, especially in infants, difficulty feeding and increased work of breathing. It affects the LOWER respiratory tract, specifically the smaller airways in the lungs right before where oxygen exchange happens (called bronchioles). So, you may also hear it referred to as “bronchiolitis.”
Most older kids handle RSV like a bad cold. But the story can be drastically different in babies. They have narrower airways, which can make congestion and inflammation a much bigger deal.
💡(Not) Fun Fact: RSV is the most common cause of lower respiratory tract infection in children under 1, and 50,000-80,000 children under age 5 are hospitalized annually in the US for RSV.
🩺 Pediatrician’s Insight: RSV is transmitted most commonly through direct contact, and it can live on surfaces for hours. So, wiping noses, using elbows to cover coughs, and frequent hand-washing are the most important things you can do to try and stop the spread at home!
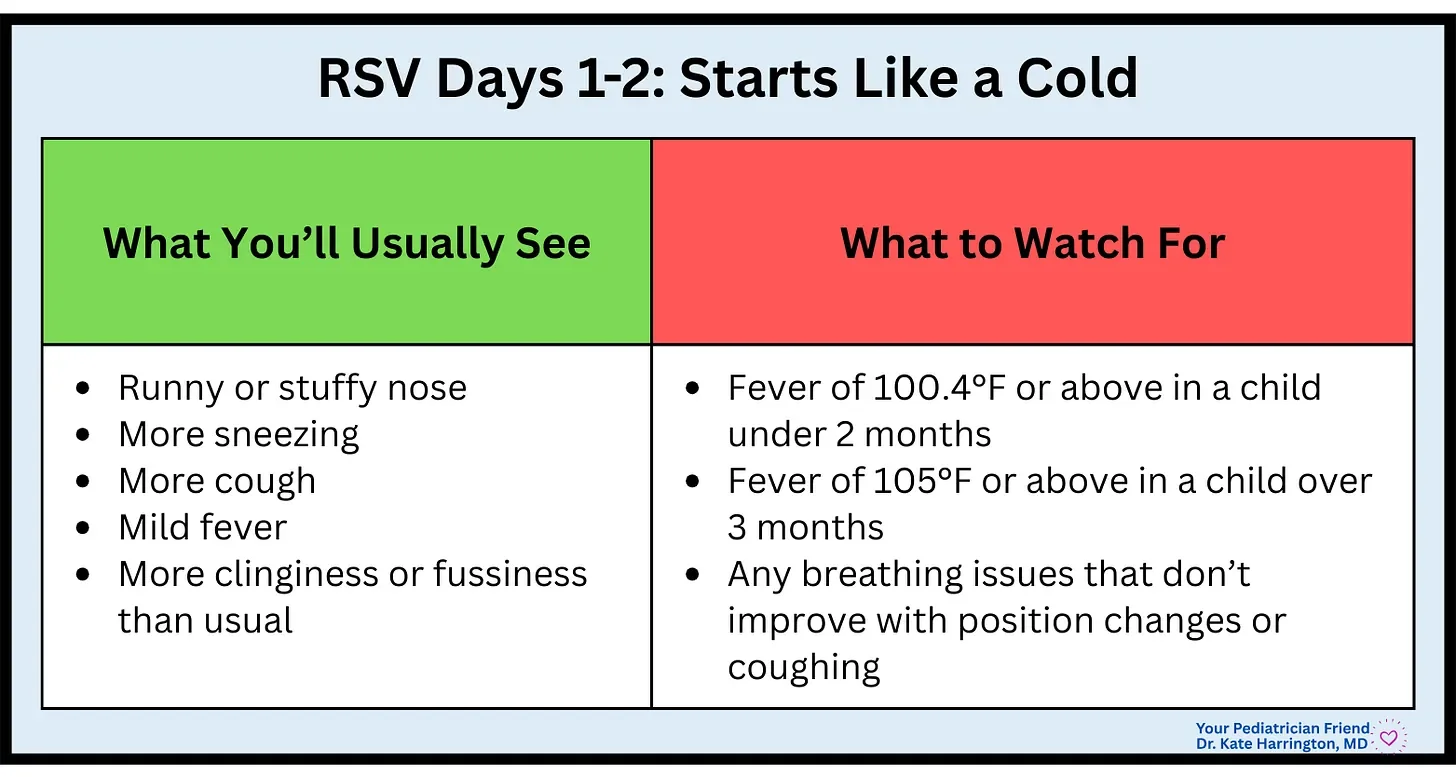
Day 1-2: It Starts Like a Cold
RSV often starts so mild that parents don’t suspect much at first. Kids usually act and feed pretty normally in these early days.
🩺 Pediatrician’s Insight: When babies have a cold, one of the most important things you can do is hydrate! This includes keeping their airways moist with nasal saline and humidity, as well as pushing oral fluids.
Days 3-4: The Hardest Stretch
This is the time when parents think, “Something definitely changed overnight.” And you are not imagining it. These are the hardest days, and the window most pediatricians worry about (especially in kids under 1). RSV truly has a “cliff” moment, where you feel like you are teetering on the edge, and just hope that you don’t fall over.
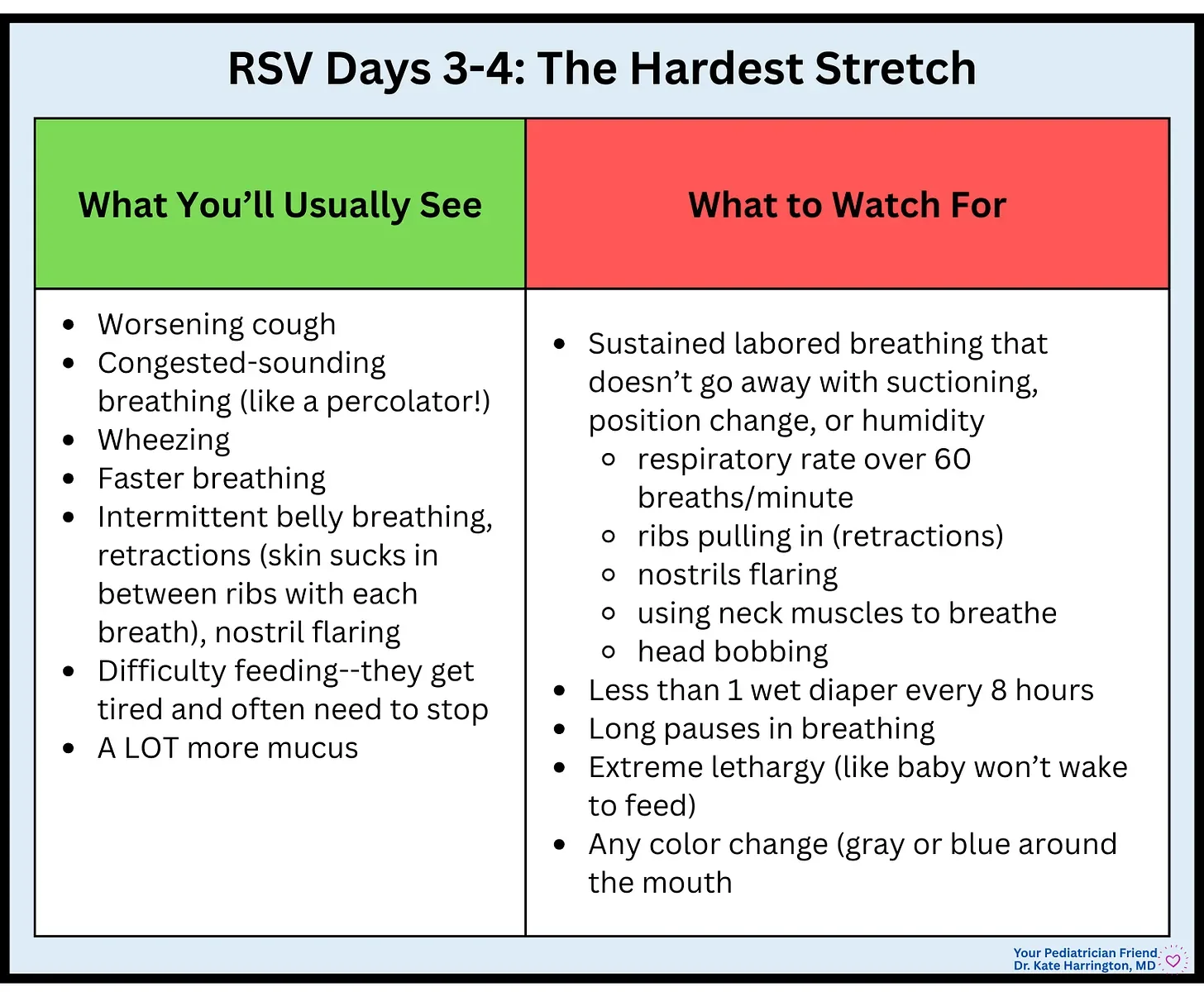
What’s happening inside the body:
Peak airway inflammation
Peak mucus production
Babies struggle with coordination of breathing and feeding because of all the mucus
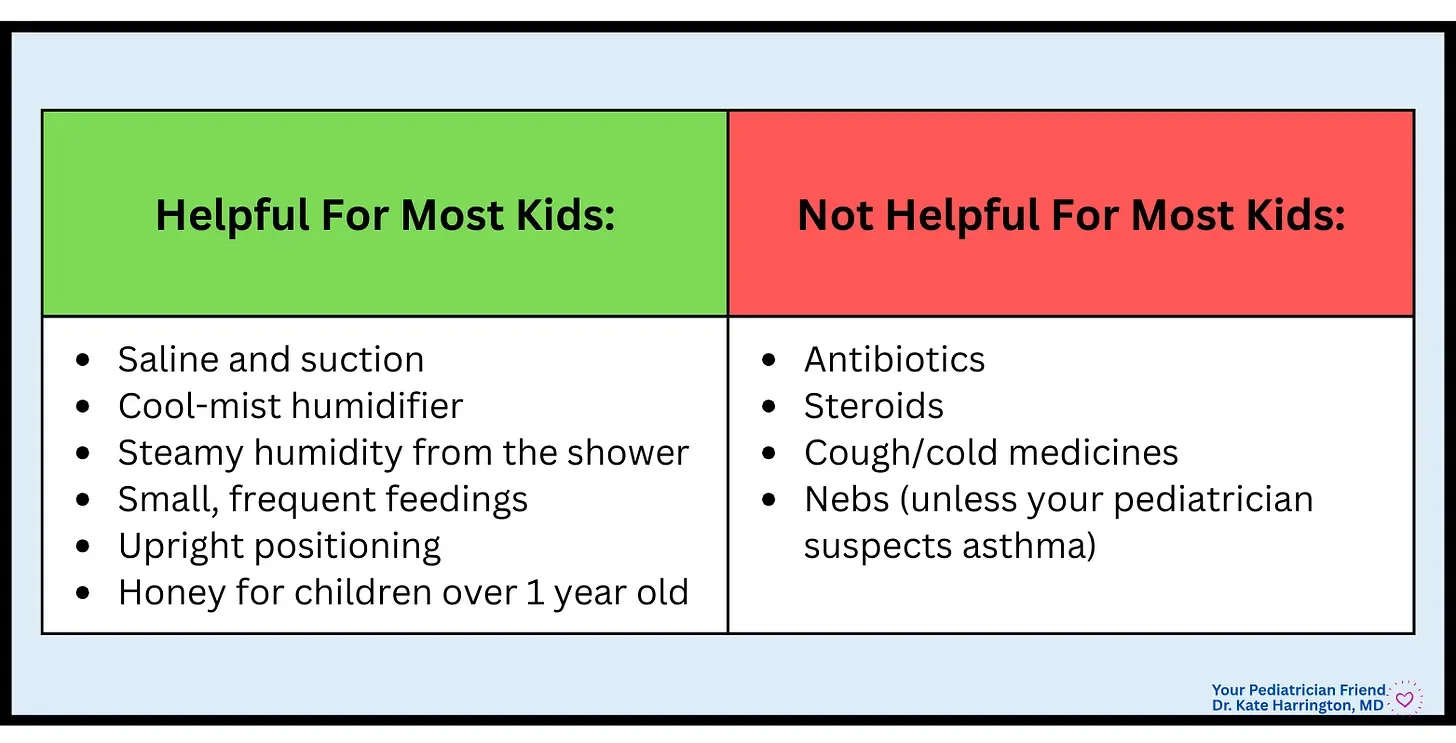
What helps at home:
Nasal saline and suction before feeds
Cool-mist humidifier
Steamy humidity from the shower
Smaller, more frequent feedings
Sitting upright for snuggles
💡Fun Fact: Pediatricians call babies with RSV “happy wheezers.” They often don’t look too sick, but sound like they are sick.
🩺 Pediatrician’s Insight: You should never be embarrassed to check in. Pediatricians are not bothered by questions, especially when it comes to breathing and your baby! So, if you are feeling unsure, reach out! A video of your child breathing can be especially helpful, and be sure to film with your child’s shirt off—we want to see how hard they are working and if there is any pulling between the ribs.
Days 5-6: The Turning Point (phew!)
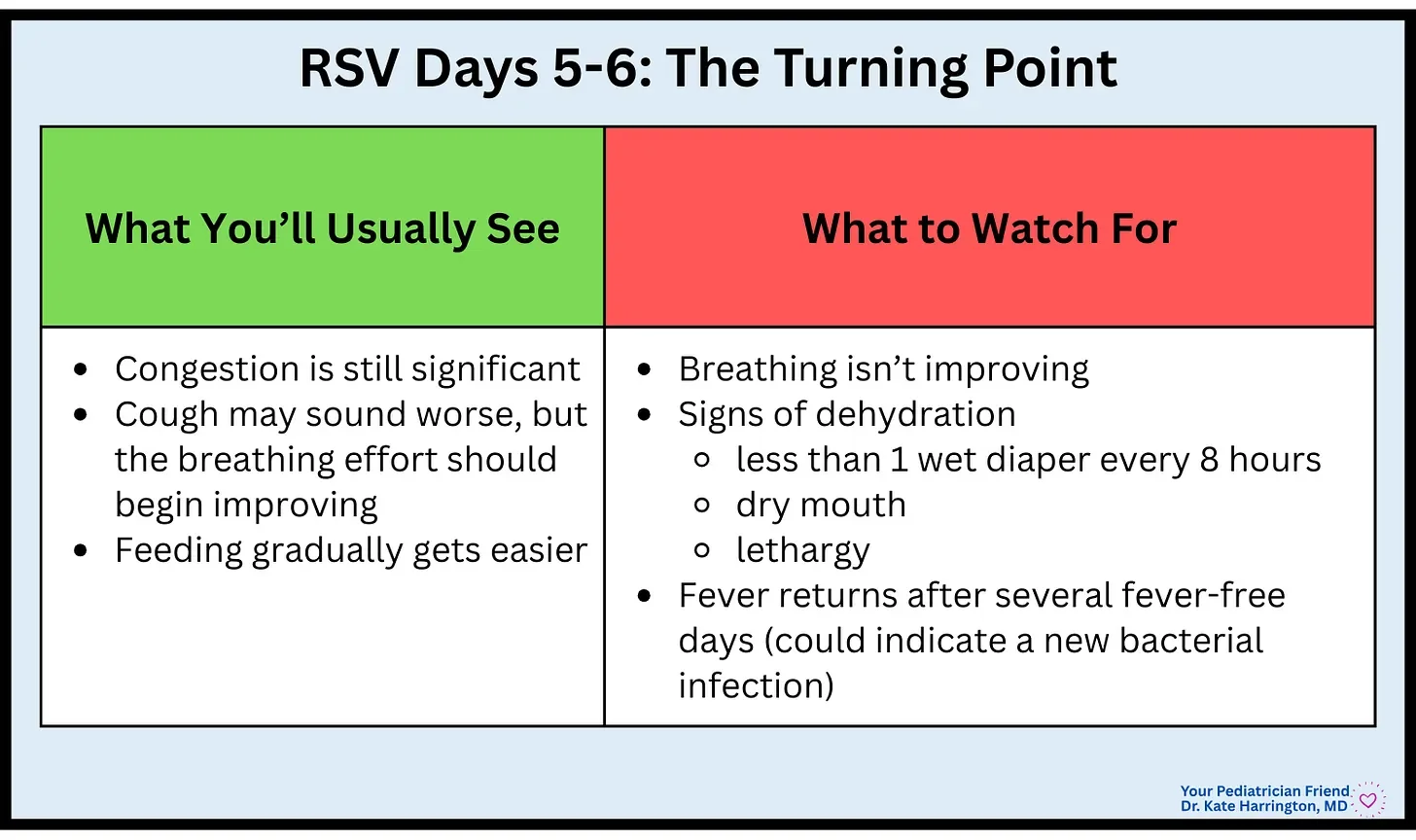
🩺 Pediatrician's Insight: This stage can be confusing because the cough may actually sound worse, but as long as the work of breathing is improving, things are moving in the right direction. The improvement is subtle: less pulling at the ribs, more sustained feedings, longer stretches of sleep.
Days 7-14 (or longer!): The Looong Cough Phase
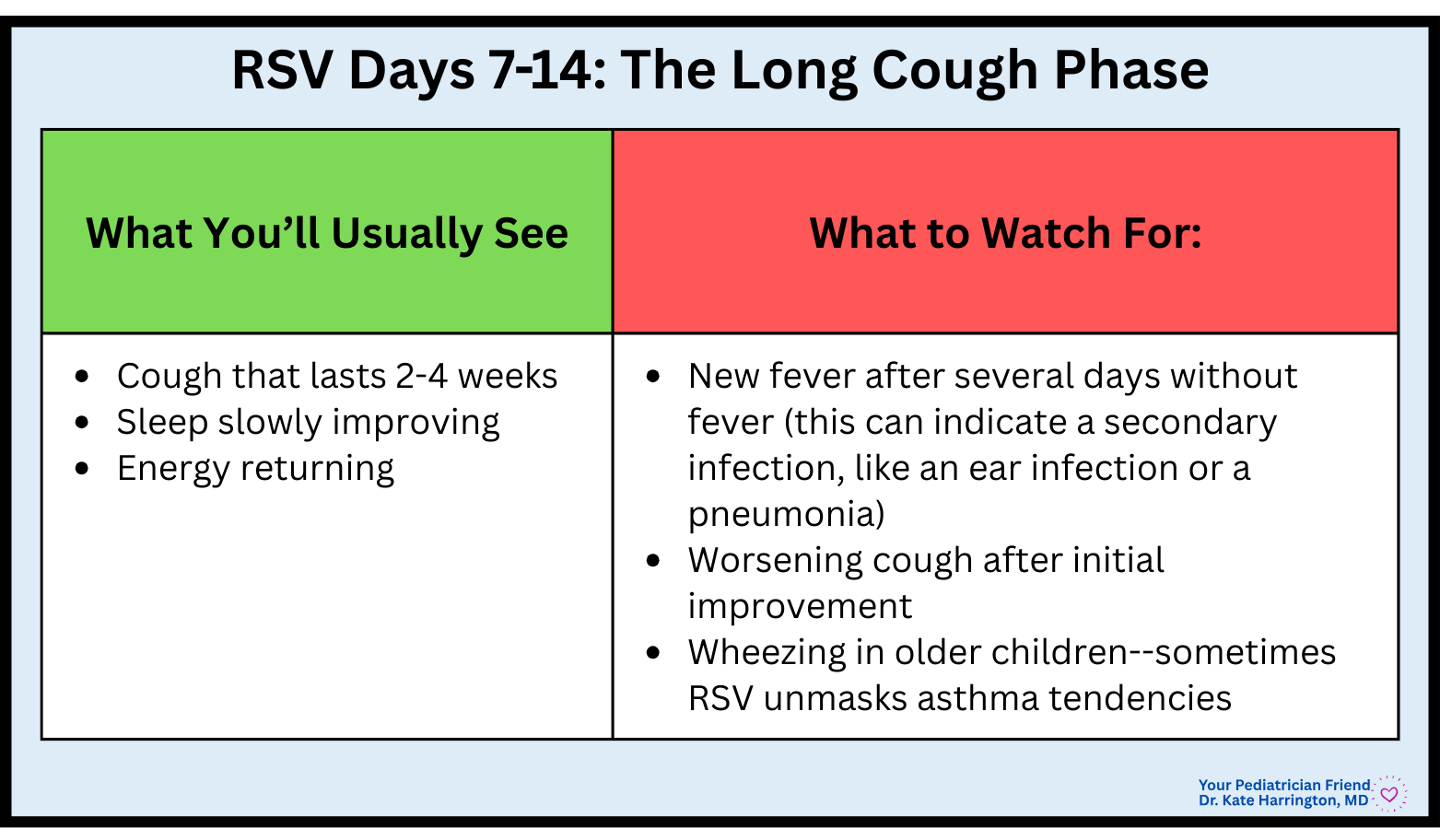
🩺 Pediatrician’s Insight: The cough lingers because little airways stay “twitchy”and inflamed long after the virus has peaked. Coughing at night may be the last symptom to go away (so maddening… know!).
When RSV Becomes An Emergency
Seek urgent medical care right away if you see:
Blue/gray color around the lips, face, or inside the mouth
Pauses in breathing that don’t get better with position changes or suctioning
Sustained breathing rate over 60 breaths per minute + retractions + neck muscle use + nostrils flaring
Inability to keep fluids down
Very sleepy or hard to wake
Fewer than 3 wet diapers in 24 hours
If your gut is screaming at you, listen to it. You know your child better than anyone else.
What Pediatricians Look for When Deciding on Hospital Care
Parents often imagine complicated treatments, but hospitalization for RSV is almost always for:
Oxygen support (needed for children with consistent oxygen saturations under 90%)
Hydration (IV fluids)
Monitoring in very young infants
Unfortunately, there are no magic fixes for RSV. No antibiotics. No cough medicines. And breathing treatments (like nebulizers) only work if a child has underlying asthma. So, we have to rely on supportive care while the body does the rest of the work.
What You Can Do To Help
Preventative tools:
RSV vaccine during pregnancy:
Clinical trial data show that maternal RSV vaccination can substantially reduce the risk of a baby being hospitalized with RSV or needing to seek other medical care for RSV in early infancy. In phase III trials, the maternal RSV vaccine reduced the risk of infant hospitalization by around 68% and the risk of severe RSV outcomes (like low oxygen or ICU care) by up to 82% in the first few months of life. (https://www.cdc.gov/rsv/hcp/vaccine-clinical-guidance/pregnant-people.html)
RSV monoclonal antibody for infants (nirsevimab):
Nirsevimab is a long-acting monoclonal antibody given as a single injection before or during an infant’s first RSV season. Clinical studies show that it can reduce RSV-associated hospitalizations by roughly 70-80% and lower the risk of severe RSV disease by around 80-85% compared with infants who do not receive it. (https://www.cdc.gov/rsv/hcp/vaccine-clinical-guidance/infants-young-children.html)
Handwashing! RSV is spread by contact, so washing hands is paramount.
Sleep and healthy foods do wonders for the immune system.
💡Fun Fact: Pediatricians have been giving RSV monoclonal antibodies to prevent severe RSV infection to high-risk infants since 1998. Before the introduction of nirsevimab, palivizumab (Synagis) was given monthly to premature infants and young children with lung and heart disease.
A Final Word of Reassurance 🩷
RSV is exhausting…physically and emotionally! The nights can feel so long and the snot is endless! But most importantly, the worry can sit heavily on your chest.
But here’s what I want you to remember: Most children get through RSV unscathed, and just need time, rest, good supportive care, and a little extra love (and you can do that!!).
You’ve got this, and there are always people here to help you. Don’t forget to rely on your helpers 💕
